
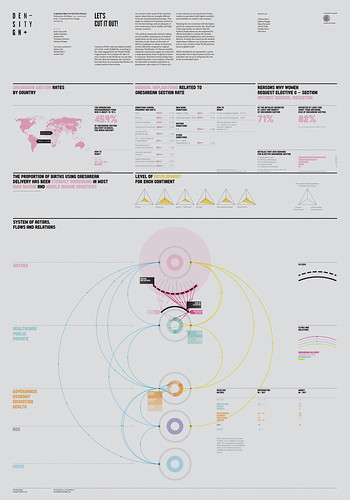
Poster: Let’s Cut It Out!
According to the value suggested by the World Health Organization, caesarean births represent approximately 15% of the world childbirths. The analysis of the data of each country in the World shows that this rate does not represent the real situation and that there is an unequal distribution of a major medical intervention. As a matter of fact the majority of countries report values which are strongly different from the recommended percentage. This implies an underuse of the caesarean section (CS) in low income settings, and an adequate or even unnecessary use in middle and high income countries.
Since medical implications can sometimes affect the choice of the route of delivery with an abuse of caesarean sections compared to the vaginal ones, the medical community started a debate on their possible consequences on the actors of the system. Worldwide, CSs that are possibly medically unnecessary appear to command a disproportionate share of global economic resources. Moreover, several studies have revealed that there is no evidence of benefit for the health of mothers and babies in populations with values of CS above 15%. On the contrary, an increased rate of intervention is associated with higher mortality and morbidity in mothers and newborns.
The study of Brazil and Chad, the two countries with the higher and lower caesarean section rate respectively, shows how medical implications are not supported by official data confirming the connection between medical implications and caesarean deliveries.
Actually, how much do the medical implications influence the caesarean section rate in every country of the World and how much at global scale? Which mechanisms are operated by a system that produces the wrong caesarean section rate and where may we act to bring back the rate to the recommended value?
Report: Have a Delivery Have a Choice
Although the global rate of caesarean sections is between 10% and 15%, the data provided by the World Health Organization show that the proportion changes significantly from country to country. There is a deep imbalance between different countries, which leads to a situation of global lack of homogeneity. Observations and studies based on structured sources and official documents allowed to determine a perspective from which to study and develop new researches.
The determination of the actors involved and their interrelations allowed us to better understand the phenomenon. The medical implications of childbirth were taken into consideration and analyzed as filters that lead to the choice of a natural or surgical solution. Our research revealed that medical implications are not the decisive factor in the choice of the type of delivery. The system around the delivery event must also be taken into consideration: from the geographical location of residence of the mother, to her economic and socio-cultural position. In the scheme of flows and relationships of this system we defined the following actors: Mother, Governance, NGO, Public Health care structure and Private Health care structure.
Video: Have a Delivery Have a Choice
Childbirth is a natural event, although a recent tendency is to intervene and turn it into a surgery.
According to the World Health Organization’s data, Caesarean births should happen in 15% of cases. This percentage, which is respected at a global level, is met only by 14 states. Caesarean section is underused in low-income countries and peaks in middle and high-income countries.
Italy is one of the countries with the highest rate. In 2012 more than 38% of births occurred via cesarean section, with a significant change from region to region. An unequal distribution of caesarean births is also among public and private hospitals and should be investigated in the type of communication these structures make. From a semantic analysis conducted on hospitals websites, it emerges how public and private hospitals deal with the topic of delivery and present themselves to potential patients.
The analysis highlights that private hospitals provide more information than public ones. Additionally, public and private structures use different and sometimes antithetical words to inform on the topic. The words used by public hospitals suggest the attitude to favor a de-medicalization of childbirth, to reduce the use of caesarean section. On the contrary, the words used by private hospitals suggest the attitude to perform an elective caesarean birth on maternal request due to fear of litigation and pressure from the patients.
On the other hand, the image private hospitals introduce themselves with also affects caesarean section rate. Rather than the traditional hospital setting, the name of clinics evokes a warm and familiar place. The imagery associated with them is also fostered by terms related to: structural and aesthetic qualities of the hospital, satisfied needs of patients and feelings associated with hospitalization, quality of medical and nursing care and any other non-hospital services.
References
Data:
World Health Organization
American Journal of Obstetrics & Gynecology
ISTAT
Ministero della Salute
Authors
Tiziana Alocci
Federico Biraghi
Elena Fiorentini
Dimitri Nube
Daniela Sonia Pessot
Sara Porco